A new report released by Inseparable offers policymakers practical tools to build and sustain a stronger mental health workforce. It includes actionable state-level strategies to expand capacity, strengthen the pipeline of new providers, support those already delivering care, and leverage data and technology to improve access and outcomes so people can get the care they need, when they need it.

Too many Americans cannot access the mental healthcare they need, due in large part to a system that lacks enough providers and oftentimes the right kinds of providers to offer the appropriate services.
With 144 million Americans living in mental health shortage areas, no state comes close to meeting demand. The highest-performing state, Rhode Island, meets just over 58 percent of its need for mental health services. In nearly half of states, at least three-quarters of required workforce capacity is simply missing.
These shortages are not inevitable. They are the result of misaligned policies, burdensome requirements, and insurance practices that make it difficult for providers to enter or remain in the field. But with the right policies, there is hope – and a clear path forward.
Several interconnected forces drive workforce shortages:
This pyramid illustrates how expanding the non-clinical workforce can
help meet more people’s needs and reduce an overreliance on more
costly, specialized services.
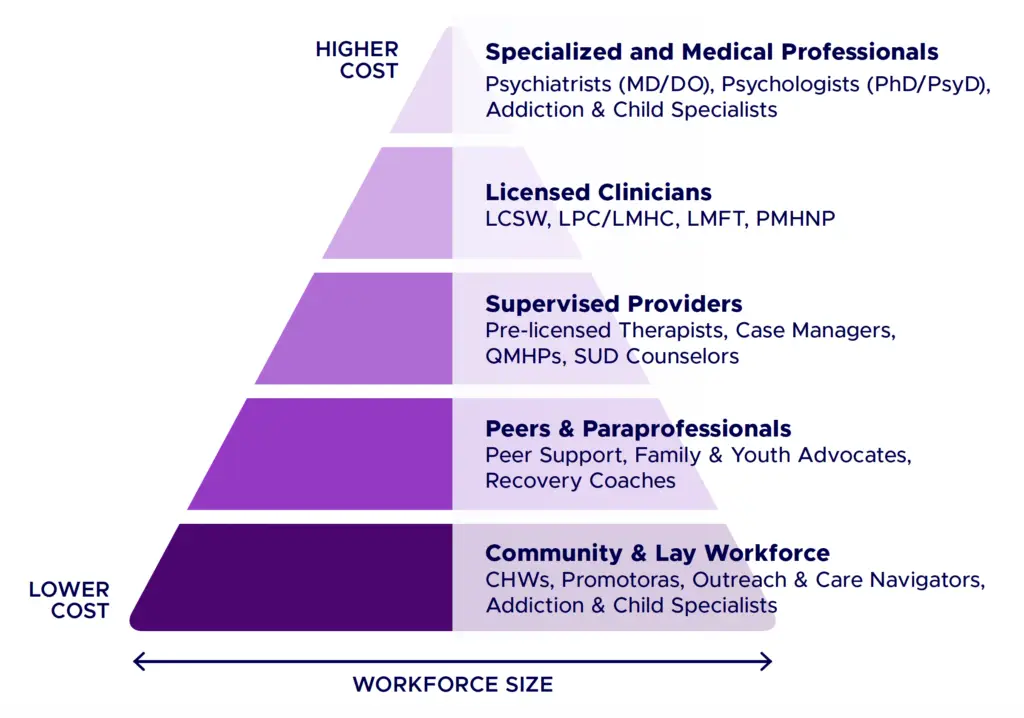
Adapted from “Enhancing the Capacity of the Mental Health and Addiction Workforce: A Framework,” February 13, 2021.
Creating an effective mental healthcare system means ensuring there are both enough providers and the right types of providers to meet demand. States can strengthen state workforce education centers, expand hands-on learning opportunities, and partner with higher education institutions to design and teach curricula that are aligned with the real-world needs of individuals with mental health and substance use challenges.
A sustainable mental health system depends on a strong pipeline of providers entering the field. Yet for many prospective clinicians, the math simply doesn’t add up: high education costs, and unpaid clinical hours make the profession financially unattainable for many. Apprenticeships, loan repayment programs, and scholarships reduce financial barriers to entering the field. Reimbursing supervised pre-licensure care allows trainees to earn income while gaining clinical hours.
Licensed clinicians such as psychologists and psychiatrists play a critical role in the mental health workforce. But many people seeking support would benefit from a broader array of providers. Peer support specialists, behavioral health technicians, and other paraprofessionals can often effectively serve individuals with less complex needs — freeing licensed clinicians to focus on those requiring more specialized treatment. States can expand capacity by creating clear credentialing pathways, integrating these roles into Medicaid, and funding the supervision structures necessary to support them.
Requiring mental health services to be reimbursed at rates comparable to physical healthcare — using Medicare rates or another external benchmark — is among the highest-impact steps a state can take. Illinois recently set a rate floor to achieve fair reimbursement rates for in-network mental health and substance use disorder services, a model other states can follow.
The Collaborative Care Model — a team-based approach that includes a primary care provider, a behavioral healthcare manager, and a consulting psychiatrist — improves outcomes, reduces long-term costs, and makes more efficient use of limited workforce capacity. Nearly 40 states cover this model in Medicaid, but only 12 require commercial health plans to cover it, leaving a significant opportunity on the table. Allowing same-day billing for physical and mental health services removes another unnecessary barrier.
States can ease administrative and financial burdens on mental health professionals by simplifying and standardizing requirements, adopting interstate licensure compacts, and dedicating agency funding to reduce processing delays.
Forty-two states participate in the Psychology Interjurisdictional Compact; 39 in the Counseling Compact; 28 in the Social Work Licensure Compact, highlighting the value of alignment.
Mental health providers are more likely to face burnout, increasing their likelihood of leaving the workforce. States can support measures that promote wellbeing among mental health providers to help them stay at work and thrive–from providing dedicated hotlines to revising discriminatory policies that deter providers from seeking care.
States need strong workforce data to identify shortage areas, align investments with need, and target solutions like loan repayment and training expansions. By facilitating data collection and partnering with educational institutions and industry stakeholders to put insights into action, states can better prepare the workforce of tomorrow.
Technology offers significant potential to support the mental health workforce—if implemented thoughtfully and with appropriate safeguards. Maintaining telehealth flexibilities can expand access, while carefully regulated AI tools can reduce administrative burden, improve care coordination, and support evidence-based digital interventions.
The mental health workforce challenge is serious, widespread, and — with the right policy choices — solvable. States that have taken targeted action are already seeing results. The Workforce Report provides state policymakers with concrete examples of what is working, a full state-by-state analysis of policy progress, and a menu of proven legislative and regulatory tools to close the gap.
Every person, regardless of where they live, what insurance they carry, or who they are, should be able to access mental healthcare when they need it. That future is within reach.
Understand your state’s progress in adopting state policies that develop the pipeline of workers, bolster the existing workforce, and harness data and technology. For insights on these policy benchmarks, read this overview.
"*" indicates required fields